
By BRIAN JOONDEPH
Synthetic intelligence is shortly changing into a core a part of healthcare operations. It drafts medical notes, summarizes affected person visits, flags irregular labs, triages messages, evaluations imaging, helps with prior authorizations, and more and more guides choice assist. AI is not only a aspect experiment in medication; it’s changing into a key interpreter of medical actuality.
That raises an essential query for physicians, directors, and policymakers alike: Is AI precisely reflecting the actual world? Or subtly reshaping it?
The information is easy. In accordance with the U.S. Census Bureau’s July 2023 estimates, about 75 % of People establish as White (together with Hispanic and non-Hispanic), round 14 % as Black or African American, roughly 6 % as Asian, and smaller percentages as Native American, Pacific Islander, or multiracial. Hispanic or Latino people, who may be of any race, make up roughly 19 % of the inhabitants.
Briefly, the information are measurable, verifiable, and accessible to the general public.
I lately carried out a easy experiment with broader implications past picture creation. I requested two prime AI image-generation platforms to supply a gaggle picture that displays the racial composition of the U.S. inhabitants based mostly on official Census knowledge.
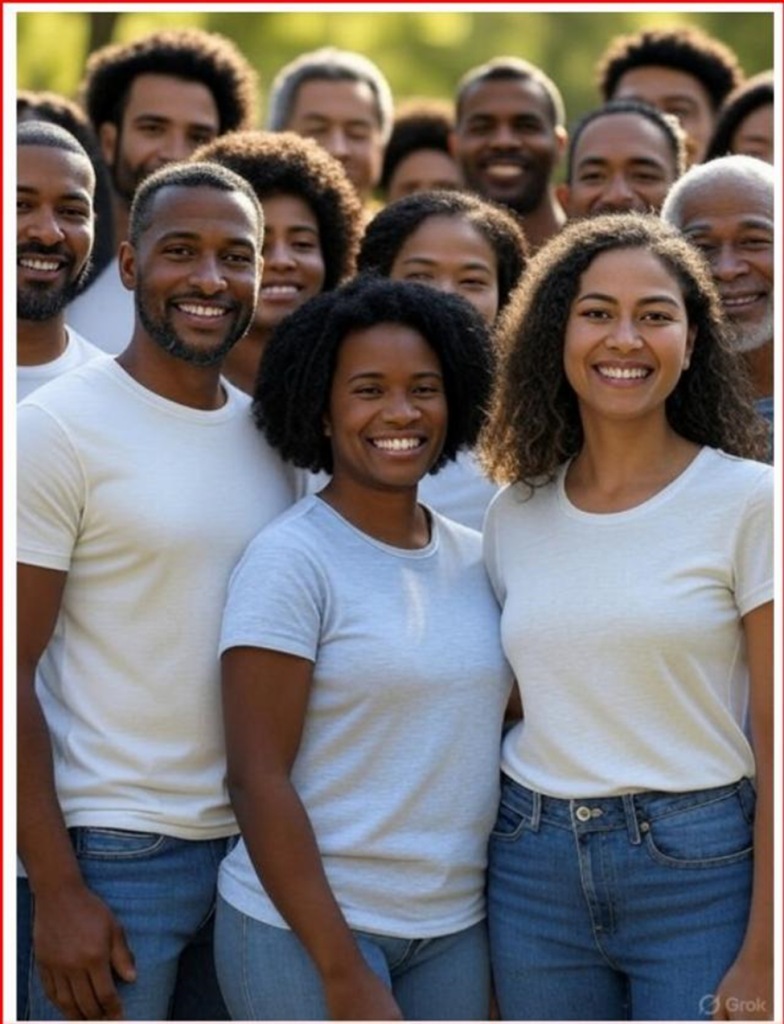
The primary system I examined was Grok 3. When requested to generate a demographically correct picture based mostly on Census knowledge, the outcome confirmed solely Black people — a whole deviation from actuality.
After extra prompts, later photographs confirmed extra variety, however White people have been nonetheless persistently underrepresented in comparison with their share of the inhabitants.

When requested, the system acknowledged that image-generation fashions may prioritize variety or purpose to handle historic underrepresentation of their outcomes.
In different phrases, the mannequin was not strictly mirroring knowledge. It was modifying illustration.
For comparability, I ran the identical immediate by way of ChatGPT 5.0. The output extra intently matched Census proportions however nonetheless wanted changes, with the ultimate picture beneath. When requested, the system defined that picture fashions may prioritize visible variety until given very particular demographic directions.

This small experiment highlights a a lot greater challenge. When an AI system is explicitly advised to reflect official demographic knowledge however finally ends up producing a model of society that’s adjusted, it’s not only a technical glitch. It reveals design selections — selections about how fashions stability the purpose of illustration with the necessity for statistical accuracy.
That pressure is especially essential in medication.
Healthcare is presently engaged in lively debate over the function of race in clinical algorithms. Lately, skilled societies and educational facilities have reexamined race-adjusted eGFR calculations, pulmonary operate take a look at reference values, and obstetric danger scoring instruments. Critics argue that utilizing race as a organic proxy might reinforce inequities. Others warn that eradicating variables with out contemplating underlying epidemiology may compromise predictive accuracy.
These debates are complicated and nuanced, however they share a core precept: medical instruments have to be clear about what variables are included, why they’re chosen, and the way they impression outcomes.
AI provides a brand new stage of opacity.
Predictive fashions now assist hospital readmission packages, sepsis alerts, imaging prioritization, and inhabitants well being outreach. Massive language fashions are being included into digital well being data to summarize notes and advocate administration plans. Machine studying methods are educated on huge datasets that inevitably mirror historic observe patterns, demographic distributions, and embedded biases.
The priority isn’t that AI will deliberately pursue ideological targets. AI methods lack consciousness. Presently a minimum of. Nevertheless, they’re educated on datasets created by people, filtered by way of algorithms developed by people, and guided by guardrails set by people. These upstream design selections have an effect on the outputs that come later. Rubbish in, rubbish out.
If image-generation instruments “rebalance” demographics to advertise variety, it’s affordable to ask whether or not medical AI instruments may also modify outputs to pursue different targets, reminiscent of fairness metrics, institutional benchmarks, regulatory incentives, or monetary constraints, even when unintentionally.
Contemplate predictive danger modeling. If an algorithm systematically adjusts output thresholds to keep away from disparate impression statistics reasonably than precisely reflecting noticed danger, clinicians may obtain deceptive alerts. If a triage mannequin is optimized to stability useful resource allocation metrics with out correct medical validation, sufferers may face unintended hurt.
Accuracy in medication isn’t beauty. It’s consequential.
Illness prevalence varies amongst populations due to genetic, environmental, behavioral, and socioeconomic elements. As an example, charges of hypertension, diabetes, glaucoma, sickle cell disease, and sure cancers differ considerably throughout demographic teams. These variations are epidemiological details, not worth judgments. Overlooking or smoothing them for the sake of representational symmetry may weaken medical precision.
None of this argues towards addressing healthcare inequities. Quite the opposite, figuring out disparities requires correct and thorough knowledge. If AI instruments blur distinctions within the identify of equity with out transparency, they might paradoxically make disparities tougher to establish and repair.
The answer is to not oppose AI integration into medication. Its benefits are vital. In ophthalmology, AI-assisted retinal picture evaluation has proven excessive sensitivity and specificity in detecting diabetic retinopathy.
In radiology, machine studying instruments can spotlight delicate findings which may in any other case go unnoticed. Scientific documentation assist can assist scale back burnout by reducing clerical workload.
The promise is actual. However so is the accountability.
Well being methods adopting AI instruments ought to require transparency relating to mannequin growth, variable significance, and insurance policies for output changes. Builders ought to reveal whether or not demographic balancing or representational modifications are built-in into coaching or inference processes.
Regulators ought to give attention to explainability requirements that allow clinicians to know not solely what an algorithm recommends, but in addition the way it reached these conclusions.
Transparency isn’t elective in healthcare; it’s important for medical accuracy and constructing belief.
Sufferers imagine that suggestions are based mostly on proof and medical judgment. If AI acts as an middleman between the clinician and affected person by summarizing data, suggesting diagnoses, stratifying danger, then its outputs have to be as true to empirical actuality as potential. In any other case, medication dangers transferring away from evidence-based observe towards narrative-driven analytics.
Synthetic intelligence has exceptional potential to enhance care supply, enhance entry, and increase diagnostic accuracy. Nevertheless, its credibility depends on alignment with verifiable details. When algorithms begin presenting the world not solely as it’s noticed however as creators imagine it ought to be proven, belief declines.
Drugs can not afford that erosion.
Information-driven care depends on knowledge constancy. If actuality turns into changeable, so does belief. And in healthcare, belief isn’t a luxurious. It’s the basis on which all the things else relies upon.
Brian C. Joondeph, MD, is a Colorado-based ophthalmologist and retina specialist. He writes continuously about synthetic intelligence, medical ethics, and the way forward for doctor observe on Dr. Brian’s Substack.